If you want to offer the possibility of a good death, you simultaneously have another obligation.
(This article was previously published in Dutch in the newspaper Nieuw Wij)
An intense and understandable emotional debate has arisen between various medical specialists and philosophers regarding requests for, and approvals of, euthanasia for people under the age of thirty. What lies behind this debate is the increasing number of requests and approvals for young people under thirty with mental health conditions. From five approved cases of euthanasia in 2020 to thirty approved cases in 2024. Notably, a significant majority (three quarters) of these individuals are women, and more than half have a diagnosis within the autism spectrum. Why is this so important? Why should alarm bells be ringing?
The possibility of assisted dying is one of the most courageous and dignified aspects of Dutch culture, something I—as a Dutch person living abroad—can only affirm. In the documentary Sista hjälpen, currently broadcast on Swedish public service television SVT, the tragedy of certain severely ill patients in Sweden becomes painfully clear. As the mother of a young man with Huntington’s disease, scraping together all her savings to fly her son to Switzerland for a dignified death.
Women may differ from men both biologically and psychologically, but we know too little to help them properly.
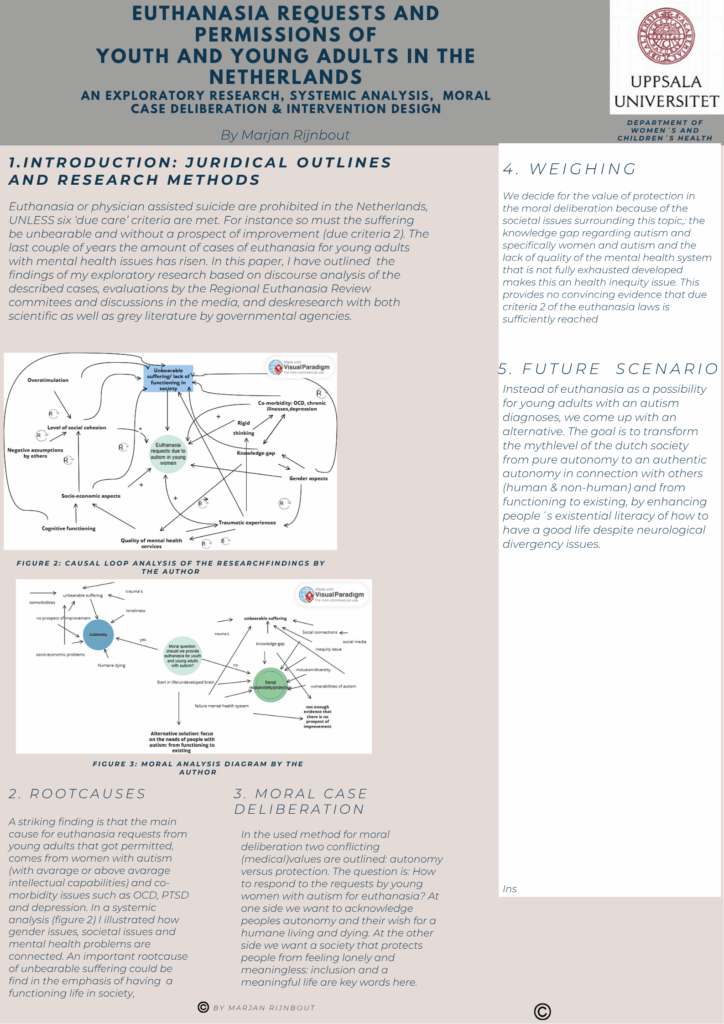
Before moving to Sweden in 2018, I worked in primary care as a humanistic and existential psychologist, philosopher, and ethicist on questions concerning assisted dying. Never, however, did I encounter a request from anyone under thirty whose suffering was based on psychiatric issues. The latest reports and the public debate surrounding these requests raise questions: why are these requests being made, and how are they evaluated? Over the past few weeks, I have immersed myself in the case descriptions on the website of the Regional Euthanasia Review Committees and carried out a systemic analysis of all the underlying aspects.
It is striking that an overwhelming majority of the approvals concern young women (around 75 percent), many of whom have autism as an underlying diagnosis. In addition, obsessions, compulsions, and post-traumatic stress disorders occur, sometimes combined with physical conditions such as chronic fatigue syndrome. The suffering is often described as “deep loneliness, lack of contact with others, feeling different, tired of life, trauma, and loss of trust in treatment.” Furthermore, disturbing and legally questionable treatment methods are mentioned, such as isolation in special rooms and involuntary electroconvulsive treatments—tens of times, sometimes over a hundred times.
There are six necessary conditions for granting assisted dying: the suffering must be unbearable and without prospect of improvement; the patient must be competent to decide, make the decision voluntarily and well-considered, and be well-informed. Additionally, no reasonable alternative may exist, an independent physician must be consulted, and the assisted dying must be carried out professionally and with great care.
In what follows, I focus primarily on the first criterion, which consists of two aspects: (1) unbearable suffering, and (2) hopelessness/lack of prospects for improvement. That psychological suffering can be unbearable is, in my view, indisputable. Most of the case descriptions are directly painful and tragic: being unable to sleep due to intrusive memories, self-harm, deep loneliness and disconnection from daily life and from others. And an intense wish to die.
But there are also problematic aspects, especially from a societal responsibility perspective. The criterion of “hopelessness” raises questions, particularly regarding gender. Three quarters of the cases concern young women, and the majority of them have autism. Even in suicide statistics, autism often plays a major role, but there it concerns primarily men.
Medical science lags behind in its knowledge of women, who often make up far too small a portion of the scientific evidence base. Women may differ biologically and psychologically from men, but we know too little to help them adequately. This also applies to women with autism, who often receive their diagnoses late because they can mask their autistic expressions. It is a sociological phenomenon: women adapt to societal expectations—something that can exhaust them over time. History shows the risks of this blind spot in medical science, such as the 19th-century diagnosis of hysteria and the dehumanizing treatments that followed. We are still far behind in our medical understanding of women.
“Autism is one of the deadliest conditions among young people—not because it directly threatens life, but because it increases the risk of suicidal thoughts.”
— Svenny Kopp
We also lag behind when it comes to autism. In people with autism, the brain functions fundamentally differently than in neurotypical individuals. This leads to increased sensitivity to stimuli: sounds, light, and even touch can be experienced very intensely. They often have significant difficulty with change and a strong need for structure. When the world feels unpredictable, this can create anxiety and uncertainty. Social cues may be harder to interpret, which complicates communication. This creates problems not only in social life, but also in school and working life. Autism could almost be described as a systemic condition, affecting the brain, social life, and the individual’s economic circumstances.
Research also shows that autism often coexists with other conditions. People with autism are at higher risk of migraines, epilepsy, and other chronic illnesses. They are also more likely to develop obsessive-compulsive disorder, depression, and ADHD. And they are more often exposed to traumatic experiences, such as bullying or sexual assault. Due to more rigid patterns of thinking, they also have fewer strategies for managing such experiences.
Autism is a lifelong, incurable condition. It is one of the deadliest conditions among young people, not because it directly threatens life, but because it greatly increases the risk of suicidal thoughts. Within the inflexible thought patterns, death may appear as a possible escape from constant suffering, and it is therefore difficult to relativize these thoughts. This raises the question: should the incurability of autism be seen as part of the criterion “hopelessness”? I would argue that the answer is no. Cure is not possible, but there are many ways to improve the quality of life for people with autism. It is not about curing, but about creating room to live.
Society’s role is crucial here. The education system and its emphasis on social functionality often place an unreasonable burden on people with neurodiversity. This is a missed opportunity: many people with autism have exceptional abilities that, when given space, can enrich both their lives and society. Research even shows that quality of life improves significantly when people with autism can immerse themselves in their special interests. It is therefore crucial that we recognize these unique abilities and create more ways of living within our society.
We see only what we recognize. Michel Foucault wrote already in 1963 in Naissance de la clinique about “the medical gaze,” how seeing, recognition, and identification are shaped by medical knowledge. Our understanding of body and mind is dominated by a medical framework. Only what can be measured and described within this epistemology becomes visible; everything else falls outside it. When men dominate both the medical profession and research, the female body and female psyche become a blind spot. And when the autistic brain is difficult to measure and categorize, their identity also remains a mystery to us.
What we need is a form of existential literacy—a capacity to navigate life’s fundamental questions.
But even if we were to catch up on the medical knowledge gap concerning women or people with autism, much lies outside this gaze. What can medicine do about loneliness? How can it help us feel connected to others, or to the world? How does it help us with questions that have no solution? The answer is often: it does not. Loneliness is not a medical diagnosis, and therefore there is no treatment. Medicine excels at action—but what do we do when action is no longer helpful?
The psychiatrist Jim van Os has written that physicians are often trained in a “vocational-school-like” way: practical and model-driven. But there is no education in wisdom. Yet it is precisely these questions that call for wisdom. What we need, I would add, is a form of existential literacy: a capacity to live with our life questions, our paradoxes, and our painful situations.
Back to the question of whether this suffering is hopeless. The way we currently organize care for young women with autism, comorbidities, and post-traumatic stress disorders may, unfortunately, make it a reality. Many of these requests come from people who are at the end of the road and have tried everything within the structures we offer. Assisted dying can be a dignified death for these individuals. And the physicians who evaluate these requests do so with as much integrity as possible. But as a society we also have a responsibility to broaden our perspective—to see beyond the tip of our medical nose. If we do not know what something is, we do not see it either. If we want to offer the possibility of a good death, we also have a moral obligation to offer young women with autism opportunities for a good life.
A brief supportive note
If you or someone you know is struggling with thoughts of self-harm, please consider reaching out to a trusted person or local health services. In most countries, you can reach emergency help by calling your local emergency number, and many places have suicide prevention hotlines available 24/7.